
Autoantibody to GNAS in Early Detection of Hepatocellular Carcinoma: A Large-Scale Sample Study Combined with Verification in Serial Sera from HCC Patients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Serum Samples
2.2. Focused Protein Microarray
2.3. Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistical Analysis
3. Results
3.1. Study Design
3.2. Performance of Autoantibody to GNAS in Sera from HCC Patients with Early and Late Stages in Discovery Phase
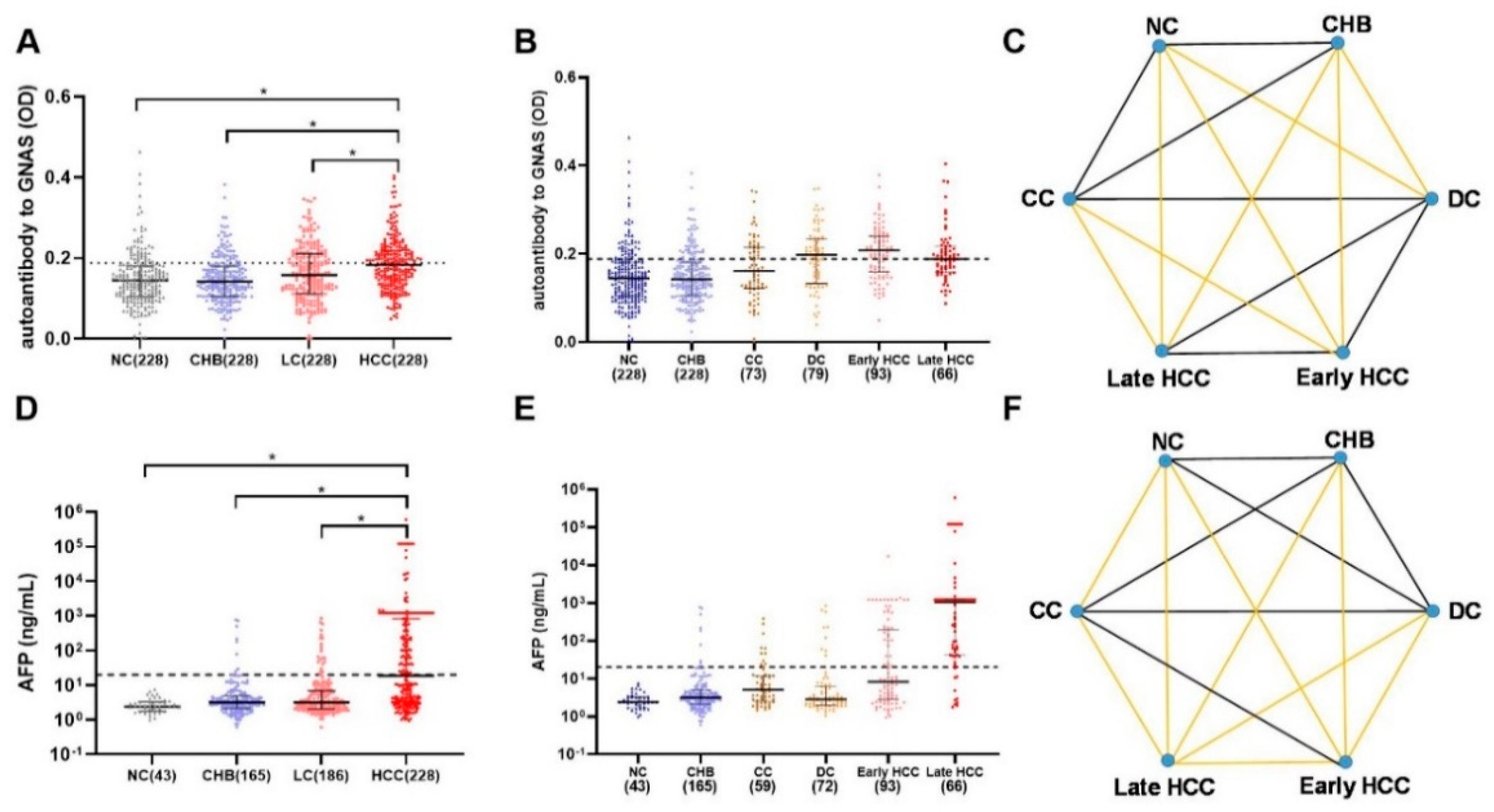
3.3. Validation in a Large-Scale Sample Set
3.4. Dynamic Change of Anti-GNAS Autoantibody in Serial Sera from 11 HCC Patients for Follow-Up Evaluation
3.5. Complementary Effects of Anti-GNAS Autoantibody on AFP in HCC Detection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Zhai, S.; Gao, J.; Wei, D.; Xue, J.; Zhou, Y.; Li, N.; Hu, L. Diagnosis of hepatocellular carcinoma using a novel anti-glycocholic acid monoclonal antibody-based method. Oncol. Lett. 2019, 17, 3103–3112. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Liu, M.; Zheng, S.-J.; Bian, D.-D.; Zhang, J.-Y.; Yao, J.; Zheng, Q.-F.; Shi, A.-M.; Li, W.-H.; Li, L.; et al. Tumor-associated autoantibodies are useful biomarkers in immunodiagnosis of α-fetoprotein-negative hepatocellular carcinoma. World J. Gastroenterol. 2017, 23, 3496–3504. [Google Scholar] [CrossRef]
- Sauzay, C.; Petit, A.; Bourgeois, A.-M.; Barbare, J.-C.; Chauffert, B.; Galmiche, A.; Houessinon, A. Alpha-foetoprotein (AFP): A multi-purpose marker in hepatocellular carcinoma. Clin. Chim. Acta 2016, 463, 39–44. [Google Scholar] [CrossRef]
- Pedersen, J.W.; Gentry-Maharaj, A.; Fourkala, E.-O.; Dawnay, A.; Burnell, M.; Zaikin, A.; Pedersen, A.E.; Jacobs, I.; Menon, U.; Wandall, H.H. Early detection of cancer in the general population: A blinded case–control study of p53 autoantibodies in colorectal cancer. Br. J. Cancer 2012, 108, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Ladd, J.; Feng, Z.; Wu, M.; Goodell, V.; Pitteri, S.J.; Li, C.I.; Prentice, R.; Hanash, S.M.; Disis, M.L. Evaluation of Known Oncoantibodies, HER2, p53, and Cyclin B1, in Prediagnostic Breast Cancer Sera. Cancer Prev. Res. 2012, 5, 1036–1043. [Google Scholar] [CrossRef] [Green Version]
- Meistere, I.; Werner, S.; Zayakin, P.; Siliņa, K.; Rulle, U.; Pismennaja, A.; Šantare, D.; Kikuste, I.; Isajevs, S.; Leja, M.; et al. The Prevalence of Cancer-Associated Autoantibodies in Patients with Gastric Cancer and Progressive Grades of Premalignant Lesions. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1564–1574. [Google Scholar] [CrossRef]
- Huangfu, M.; Xu, S.; Li, S.; Sun, B.; Lee, K.-H.; Liu, L.; Sun, S. A panel of autoantibodies as potential early diagnostic serum biomarkers in patients with cervical cancer. Tumor Biol. 2016, 37, 8709–8714. [Google Scholar] [CrossRef]
- Lowe, F.J.; Shen, W.; Zu, J.; Li, J.; Wang, H.; Zhang, X.; Zhong, L. A novel autoantibody test for the detection of pre-neoplastic lung lesions. Mol. Cancer 2014, 13, 78. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Wang, J.; Li, J.; Zhang, H.; Guo, S.; Yan, M.; Zhu, Z.; Lan, B.; Ding, Y.; Xu, M.; et al. Identification of Serum Biomarkers for Gastric Cancer Diagnosis Using a Human Proteome Microarray. Mol. Cell. Proteom. 2016, 15, 614–623. [Google Scholar] [CrossRef] [Green Version]
- Tan, E.M.; Zhang, J. Autoantibodies to tumor-associated antigens: Reporters from the immune system. Immunol. Rev. 2008, 222, 328–340. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-Y.; Tan, E.M. Autoantibodies to tumor-associated antigens as diagnostic biomarkers in hepatocellular carcinoma and other solid tumors. Expert Rev. Mol. Diagn. 2010, 10, 321–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, I.K.; Parsy-Kowalska, C.B.; Chapman, C.J. Autoantibodies: Opportunities for Early Cancer Detection. Trends Cancer 2017, 3, 198–213. [Google Scholar] [CrossRef]
- Qin, J.; Wang, S.; Shi, J.; Ma, Y.; Wang, K.; Ye, H.; Zhang, X.; Wang, P.; Wang, X.; Song, C.; et al. Using recursive partitioning approach to select tumor-associated antigens in immunodiagnosis of gastric ade-nocarcinoma. Cancer Sci. 2019, 110, 1829–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, L.; Ren, P.; Liu, M.; Imai, H.; Tan, E.M.; Zhang, J.-Y. Using immunomic approach to enhance tumor-associated autoantibody detection in diagnosis of hepatocellular carcinoma. Clin. Immunol. 2014, 152, 127–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Li, M.; Qin, J.; Sun, G.; Dai, L.; Wang, P.; Ye, H.; Shi, J.; Cheng, L.; Yang, Q.; et al. Serological Biomarkers for Early Detection of Hepatocellular Carcinoma: A Focus on Autoantibodies against Tumor-Associated Antigens Encoded by Cancer Driver Genes. Cancers 2020, 12, 1271. [Google Scholar] [CrossRef]
- Bar-Shavit, R.; Maoz, M.; Kancharla, A.; Kumar Nag, J.; Agranovich, D.; Grisaru-Granovsky, S.; Uziely, B. G Protein-Coupled Receptors in Cancer. Int. J. Mol. Sci. 2016, 17, 1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parish, A.J.; Nguyen, V.; Goodman, A.M.; Murugesan, K.; Frampton, G.M.; Kurzrock, R. GNAS, GNAQ, and GNA11 alterations in patients with diverse cancers. Cancer 2018, 124, 4080–4089. [Google Scholar] [CrossRef] [Green Version]
- Landis, C.A.; Masters, S.B.; Spada, A.; Pace, A.M.; Bourne, H.R.; Vallar, L. GTPase inhibiting mutations activate the α chain of Gs and stimulate adenylyl cyclase in human pituitary tumours. Nat. Cell Biol. 1989, 340, 692–696. [Google Scholar] [CrossRef]
- Lyons, J.; Landis, C.A.; Harsh, G.; Vallar, L.; Grünewald, K.; Feichtinger, H.; Duh, Q.-Y.; Clark, O.H.; Kawasaki, E.; Bourne, H.R.; et al. Two G Protein Oncogenes in Human Endocrine Tumors. Science 1990, 249, 655–659. [Google Scholar] [CrossRef]
- Ritterhouse, L.L.; Vivero, M.; Mino-Kenudson, M.; Sholl, L.M.; Iafrate, A.J.; Nardi, V.; Dong, F. GNAS mutations in primary mucinous and non-mucinous lung adenocarcinomas. Mod. Pathol. 2017, 30, 1720–1727. [Google Scholar] [CrossRef]
- Hara, K.; Saito, T.; Hayashi, T.; Yimit, A.; Takahashi, M.; Mitani, K.; Takahashi, M.; Yao, T. A mutation spectrum that includes GNAS, KRAS and TP53 may be shared by mucinous neoplasms of the appendix. Pathol. -Res. Pract. 2015, 211, 657–664. [Google Scholar] [CrossRef]
- Fecteau, R.E.; Lutterbaugh, J.; Markowitz, S.D.; Willis, J.; Guda, K. GNAS Mutations Identify a Set of Right-Sided, RAS Mutant, Villous Colon Cancers. PLoS ONE 2014, 9, e87966. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Matthaei, H.; Maitra, A.; Dal Molin, M.; Wood, L.D.; Eshleman, J.R.; Goggins, M.; Canto, M.I.; Schulick, R.D.; Edil, B.H.; et al. Recurrent GNAS Mutations Define an Unexpected Pathway for Pancreatic Cyst Development. Sci. Transl. Med. 2011, 3, 92ra66. [Google Scholar] [CrossRef] [Green Version]
- Kalfa, N.; Lumbroso, S.; Boulle, N.; Guiter, J.; Soustelle, L.; Costa, P.; Chapuis, H.; Baldet, P.; Sultan, C. Activating mutations of Gsalpha in kidney cancer. J. Urol. 2006, 176, 891–895. [Google Scholar] [CrossRef]
- Jin, X.; Zhu, L.; Cui, Z.; Tang, J.; Xie, M.; Ren, G. Elevated expression of GNAS promotes breast cancer cell proliferation and migration via the PI3K/AKT/Snail1/E-cadherin axis. Clin. Transl. Oncol. 2019, 21, 1207–1219. [Google Scholar] [CrossRef]
- Ding, H.; Zhang, X.; Su, Y.; Jia, C.; Dai, C. GNAS promotes inflammation-related hepatocellular carcinoma progression by promoting STAT3 activation. Cell. Mol. Biol. Lett. 2020, 25, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Sun, H.-C.; Wang, Z.; Cong, W.-M.; Wang, J.-H.; Zeng, M.-S.; Yang, J.-M.; Bie, P.; Liu, L.-X.; Wen, T.-F.; et al. Guidelines for Diagnosis and Treatment of Primary Liver Cancer in China (2017 Edition). Liver Cancer 2018, 7, 235–260. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.S.; Pawlik, T.M.; Vauthey, J.N. 8th Edition of the AJCC Cancer Staging Manual: Pancreas and Hepatobiliary Cancers. Ann. Surg. Oncol. 2018, 25, 845–847. [Google Scholar] [CrossRef] [PubMed]
- EASL. Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Wang, X.; Qiu, C.; Qin, J.; Wang, K.; Sun, G.; Jiang, D.; Li, J.; Wang, L.; Shi, J.; et al. Using protein microarray to identify and evaluate autoantibodies to tumor-associated antigens in ovarian cancer. Cancer Sci. 2021, 112, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Li, T.-Y.; Yang, Y.; Zhou, G.; Tu, Z.-K. Immune suppression in chronic hepatitis B infection associated liver disease: A review. World J. Gastroenterol. 2019, 25, 3527–3537. [Google Scholar] [CrossRef]
- Teng, C.-F.; Yu, C.-H.; Chang, H.-Y.; Hsieh, W.-C.; Wu, T.-H.; Lin, J.-H.; Wu, H.C.; Jeng, L.-B.; Su, I.-J. Chemopreventive Effect of Phytosomal Curcumin on Hepatitis B Virus-Related Hepatocellular Carcinoma in A Transgenic Mouse Model. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Levrero, M.; Zucman-Rossi, J. Mechanisms of HBV-induced hepatocellular carcinoma. J. Hepatol. 2016, 64, S84–S101. [Google Scholar] [CrossRef]
- Ringelhan, M.; Pfister, D.; O’Connor, T.; Pikarsky, E.; Heikenwalder, M. The immunology of hepatocellular carcinoma. Nat. Immunol. 2018, 19, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Neuveut, C.; Wei, Y.; Buendia, M.A. Mechanisms of HBV-related hepatocarcinogenesis. J. Hepatol. 2010, 52, 594–604. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, F.; Rinaldi, A.; Marchese, G.; Coviello, E.; Sellitto, A.; Cordella, A.; Giurato, G.; Nassa, G.; Ravo, M.; Tarallo, R.; et al. Specific patterns of PIWI-interacting small noncoding RNA expression in dysplastic liver nodules and hepatocellular carcinoma. Oncotarget 2016, 7, 54650–54661. [Google Scholar] [CrossRef]
- Harris, P.S.; Hansen, R.M.; Gray, M.E.; Massoud, O.I.; McGuire, B.M.; Shoreibah, M.G. Hepatocellular carcinoma surveillance: An evidence-based approach. World J. Gastroenterol. 2019, 25, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Hallouch, O.; Chernyak, V.; Kamaya, A.; Sirlin, C.B. Epidemiology of hepatocellular carcinoma: Target population for surveillance and diagnosis. Abdom. Radiol. 2018, 43, 13–25. [Google Scholar] [CrossRef]
- Kokudo, N.; Hasegawa, K.; Akahane, M.; Igaki, H.; Izumi, N.; Ichida, T.; Uemoto, S.; Kaneko, S.; Kawasaki, S.; Ku, Y.; et al. Evidence-based Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2013 update (3rd JSH-HCC Guidelines). Hepatol. Res. 2015, 45. [Google Scholar] [CrossRef]
- Kojiro, M.; Roskams, T. Early Hepatocellular Carcinoma and Dysplastic Nodules. Semin. Liver Dis. 2005, 25, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, A.; Jin, D.X.; De Marco, L.; Laitman, Y.; Friedman, E. Activating genomic alterations in the Gs alpha gene ( GNAS ) in 274 694 tumors. Genes Chromosom. Cancer 2020, 59, 503–516. [Google Scholar] [CrossRef]
- Lin, Y.-L.; Ma, R.; Li, Y. The biological basis and function of GNAS mutation in pseudomyxoma peritonei: A review. J. Cancer Res. Clin. Oncol. 2020, 146, 2179–2188. [Google Scholar] [CrossRef]
- Nault, J.C.; Fabre, M.; Couchy, G.; Pilati, C.; Jeannot, E.; Van Nhieu, J.T.; Saint-Paul, M.-C.; De Muret, A.; Redon, M.-J.; Buffet, C.; et al. GNAS-activating mutations define a rare subgroup of inflammatory liver tumors characterized by STAT3 activation. J. Hepatol. 2012, 56, 184–191. [Google Scholar] [CrossRef]
- Tyers, M.; Mann, M. From genomics to proteomics. Nature 2003, 422, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D. Does the immune system see tumors as foreign or self? Annu. Rev. Immunol. 2003, 21, 807–839. [Google Scholar] [CrossRef]
- O’Donnell, J.S.; Teng, M.W.L.; Smyth, M.J. Cancer immunoediting and resistance to T cell-based immunotherapy. Nat. Rev. Clin. Oncol. 2019, 16, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Y.; Megliorino, R.; Peng, X.X.; Tan, E.M.; Chen, Y.; Chan, E.K. Antibody detection using tumor-associated antigen mini-array in immunodiagnosing human hepatocel-lular carcinoma. J. Hepatol. 2007, 46, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Welberry, C.; Macdonald, I.; McElveen, J.; Parsy-Kowalska, C.; Allen, J.; Healey, G.; Irving, W.; Murray, A.; Chapman, C. Tumor-associated autoantibodies in combination with alpha-fetoprotein for detection of early stage hepatocellular carcinoma. PLoS ONE 2020, 15, e0232247. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.T.; Sato, M.M.; Wong, L.L.; Tiirikainen, M.; Kwee, S.A. Clinical and molecular sub-classification of hepatocellular carcinoma relative to alpha-fetoprotein level in an Asia-Pacific island cohort. Hepatoma Res. 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discovery Phase | Validation Phase | |||||
|---|---|---|---|---|---|---|
| HCC | NC | HCC | NC | LC | CHB | |
| N | 96 | 49 | 228 | 228 | 228 | 228 |
| Gender, n (%) | ||||||
| Male | 79 (82.3) | 22 (44.9) | 187 (82.0) | 187 (82.0) | 187 (82.0) | 179 (78.5) |
| Female | 17 (17.7) | 27 (55.1) | 41 (18.0) | 41 (18.0) | 41 (18.0) | 49 (21.5) |
| Age, years | ||||||
| Range | 37–78 | 20–71 | 20–75 | 21–73 | 23–75 | 23–79 |
| Mean ± SD | 56.7 ± 9.3 | 40.1 ± 12.8 | 52.3 ± 10.7 | 51.4 ± 10.2 | 52.2 ± 10.5 | 45.2 ± 11.1 |
| AFP, n (%) | ||||||
| AFP (+) | 56 (58.3) | 0 (0) | 113 (49.6) | 0 (0) | 21 (9.2) | 8 (3.5) |
| AFP (−) | 40 (41.7) | 49 (100) | 115 (50.4) | 43 (18.9) | 165 (72.4) | 157 (68.9) |
| NA | 0 (0) | 0 (0) | 0 (0) | 185 (81.1) | 42 (18.4) | 61 (26.8) |
| HCC stage, n (%) | ||||||
| Early-stage | 53 (55.2) | 93 (40.8) | ||||
| Late-stage | 43 (44.8) | 66 (28.9) | ||||
| NA | 0 (0) | 69 (30.3) | ||||
| LC stage, n (%) | ||||||
| CC | 73 (30.0) | |||||
| DC | 79 (34.7) | |||||
| NA | 76 (33.3) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Wang, K.; Qiu, C.; Wang, B.; Zhang, X.; Ma, Y.; Dai, L.; Zhang, J.-Y. Autoantibody to GNAS in Early Detection of Hepatocellular Carcinoma: A Large-Scale Sample Study Combined with Verification in Serial Sera from HCC Patients. Biomedicines 2022, 10, 97. https://doi.org/10.3390/biomedicines10010097
Wang X, Wang K, Qiu C, Wang B, Zhang X, Ma Y, Dai L, Zhang J-Y. Autoantibody to GNAS in Early Detection of Hepatocellular Carcinoma: A Large-Scale Sample Study Combined with Verification in Serial Sera from HCC Patients. Biomedicines. 2022; 10(1):97. https://doi.org/10.3390/biomedicines10010097
Chicago/Turabian StyleWang, Xiao, Keyan Wang, Cuipeng Qiu, Bofei Wang, Xiaojun Zhang, Yangcheng Ma, Liping Dai, and Jian-Ying Zhang. 2022. "Autoantibody to GNAS in Early Detection of Hepatocellular Carcinoma: A Large-Scale Sample Study Combined with Verification in Serial Sera from HCC Patients" Biomedicines 10, no. 1: 97. https://doi.org/10.3390/biomedicines10010097